EMDR for Depression: How EMDR Helps Your Brain Unstick Old Pain
Short answer: Yes—EMDR (Eye Movement Desensitization and Reprocessing) can be used to treat depression. It targets the memory networks and negative beliefs that keep mood symptoms looping. Instead of retelling every detail, you and your therapist use brief sets of eye movements, taps, or tones to help the brain reprocess stuck experiences so your nervous system can stand down and your mood has room to lift.
Depression can feel like a fog that won’t move. For many people, that fog is tied to old events—losses, failures, betrayals, or years of quiet criticism—that built up into beliefs like “I’m powerless” or “I’m not good enough.” EMDR focuses on those belief‑memory links. When the brain finishes what it couldn’t finish back then, the emotional charge drops. People often notice less rumination, more energy, and a wider window for hope.
EMDR isn’t magic; it’s method. Your therapist follows a structured, eight‑phase protocol that keeps you safe, grounded, and in control of the pace.
How does EMDR therapy work for depressive symptoms?

EMDR uses bilateral stimulation—guided eye movements, taps, or tones—to help the brain connect what you felt back then with what you know now. Think of it like hitting “resume processing” on a file the brain had to leave unfinished.
Under the hood is the Adaptive Information Processing (AIP) model. It says distressing experiences can get stored in a raw, unprocessed way. When something in the present bumps that old file—like a setback at work—it reactivates the same emotions and body sensations, which can fuel low mood and hopelessness. EMDR helps link the old file to more accurate, current information, so the brain files it away correctly.
In practice, you briefly bring a target memory or theme to mind (images, thoughts, body sensations), then follow short sets of eye movements. After each set, you notice what comes up next. The brain does the associating. You don’t have to force insights; they tend to arise naturally.
Why this helps depression:
- Rumination eases when the “unfinished” charge behind it settles.
- Guilt and shame soften as rigid beliefs (“It was all my fault”) update.
- Anhedonia and low energy often improve as the nervous system spends less effort bracing for old pain.
Isn’t EMDR just for trauma?
EMDR began in trauma treatment, but you don’t need a single big event to benefit. Many people with depression carry cumulative stress: repeated put‑downs, chronic uncertainty, or small losses that add up. We can target those patterns, not only one moment in time. This broader use is echoed in a narrative review on EMDR within affective disorders.
Targets are flexible. For some, it’s a clear incident (a breakup, a layoff). For others, it’s a thread—like a lifelong sense of being “the problem.” EMDR lets us work with both kinds of material, always at a pace that keeps you within your coping range.
If your depression is tangled with anxiety, perfectionism, or relationship stress, EMDR can be tailored to address those links in the same plan.
What does the evidence say?
Research on EMDR for depressive disorders has grown over the past decade. You’ll see support from randomized controlled trials and systematic reviews/meta‑analyses.
- Symptom reduction: Multiple trials report meaningful drops on standard depression (that is, people feel better) measures like the Beck Depression Inventory.
- Durability: Gains often hold at follow‑up.
- Efficiency: When targets are well chosen, several reports note improvement over 4–8 sessions.
- Fit with co‑occurring issues: When depression intertwines with trauma or ongoing stress, outcomes are stronger in plans that address both, a point emphasized in a review of EMDR in affective disorders.
When is EMDR not the first step?
Safety comes first. Your therapist will stabilize and coordinate care before reprocessing if there’s acute suicidality, unmanaged mania or psychosis, severe dissociation, or unstable substance use. Readiness usually means you have grounding skills, a basic safety plan, and support between sessions. If you’re on medication, EMDR can proceed in collaboration with your prescriber.
What to expect in a short EMDR plan (4–8+ sessions)
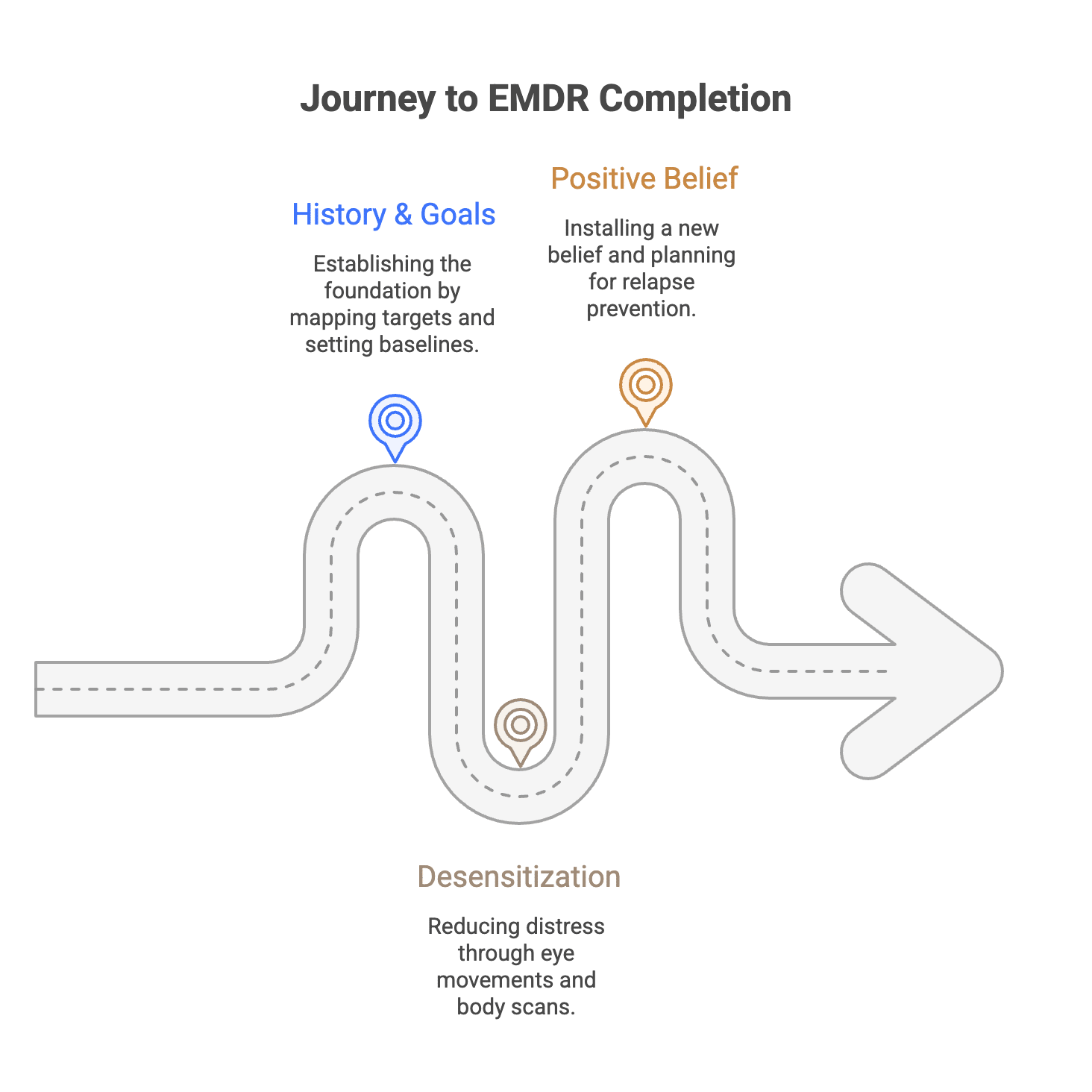
Session 1–2: History, goals, and safety. We map targets (events, themes, or beliefs), teach simple regulation skills, and set baselines—Subjective Units of Distress (SUD) and how true a positive belief feels (Validity of Cognition, VoC).
Session 3–6: Desensitization and reprocessing. You bring the target to mind while following eye movements. We check SUD as it drops, notice body sensations, and follow where the mind goes. When distress is low, we do a brief body scan to clear leftover tension.
Session 7–8+: Installing a positive belief (for example, from “I’m powerless” to “I can handle this now”), then relapse‑prevention planning: triggers to watch, skills to keep, and when to come back for a tune‑up.
EMDR vs. other effective options
EMDR plays well with others. Many people combine it with CBT or behavioral activation to rebuild daily structure and mindfulness to catch spirals early. Antidepressant medication can support sleep and energy while EMDR reduces the emotional load. The right mix depends on your history, preferences, and medical picture.
Finding a qualified EMDR therapist
Look for formal EMDR training, ongoing supervision, and a collaborative style. Ask how they pace work, how they handle stuck points, and how you’ll measure change together. You should feel respected, informed, and in charge of the throttle.
Bottom line: Depression isn’t laziness or weakness. When old pain drives today’s low mood, EMDR gives your brain a structured way to finish the unfinished—and move forward with more ease.
Frequently Asked Questions about EMDR for Depression
What is EMDR therapy and how does it work for depression?
EMDR therapy (Eye Movement Desensitization and Reprocessing) is a psychotherapeutic treatment originally developed for post traumatic stress disorder (PTSD). It involves bilateral stimulation, such as guided eye movements, to help reprocess traumatic memories and negative belief systems that contribute to depression symptoms. By targeting unresolved trauma and stressful life events, EMDR helps depressive patients reduce negative thoughts and improve emotional regulation.
Can EMDR be effective for different types of depression?
Yes, EMDR has been shown to be an effective treatment for various depressive disorders, including major depressive disorder, recurrent depression, persistent depressive disorder, and chronic depression. It is especially beneficial for depressive patients whose symptoms are linked to childhood trauma, emotional abuse, or other adverse childhood experiences.
How many EMDR sessions are typically needed to see improvement?
Clinical trials and randomized controlled trials suggest that significant improvement in depression symptoms can often be seen after 4 to 8 EMDR sessions. However, the number of sessions may vary depending on individual needs, severity of depression, and presence of comorbid PTSD or other mental health conditions.
Is EMDR therapy used as a standalone treatment or combined with other therapies?
EMDR therapy can be used both as a standalone effective treatment and as an adjunctive treatment alongside psychological therapies like cognitive therapy (CBT), medication, or behavioral activation. Combining EMDR with other treatments can enhance outcomes, especially in cases of treatment-resistant depression or when traumatic experiences are involved.
Are there any exclusion criteria for EMDR therapy in depressed patients?
Yes, certain exclusion criteria apply to ensure safety and treatment effectiveness. EMDR is generally not recommended as the first step for patients with acute suicidality, unmanaged bipolar disorder, psychosis, severe dissociation, or unstable substance use. Therapists assess readiness carefully and may stabilize patients before starting EMDR intervention.
What does previous research say about the effectiveness of EMDR for depression?
Previous research, including systematic reviews and meta-analyses, supports EMDR’s effectiveness in reducing depression symptoms and preventing relapse. Studies from the European Depression EMDR Network and other clinical psychology research groups highlight significant improvement and complete remission in many depressive patients following EMDR reprocessing therapy.
How does EMDR impact the brain in treating depression?
EMDR influences brain regions such as the prefrontal cortex and helps regulate the HPA axis, which are involved in emotional regulation and stress response. By reprocessing distressing memories and negative belief systems, EMDR promotes neuroplasticity and reduces the emotional burden that sustains depressive episodes.